Idiopathic Intracranial Hypertension(IIH)
The human brain is surrounded by cerebrospinal fluid (CSF), which cushions and protects it within the skull. In IIH, for reasons not fully understood, there is increased production or reduced absorption of CSF, leading to abnormal pressure buildup. This heightened pressure can compress the optic nerves and other brain structures, causing headache, vision problems, and in some cases permanent visual loss if untreated.
The term “idiopathic” indicates that no specific underlying cause is identifiable, although several factors may contribute to the condition.
Causes and Risk Factors
While IIH is termed idiopathic, certain conditions and risk factors are commonly associated with its development:
- Obesity: The most significant risk factor; excess body weight can influence CSF dynamics and venous drainage.
- Female gender: Women between 20–45 years are more frequently affected.
- Hormonal changes: Linked to oral contraceptives, pregnancy, or hormonal disorders such as polycystic ovarian syndrome (PCOS).
- Medications: Certain drugs may increase intracranial pressure, including tetracycline antibiotics, vitamin A derivatives (like isotretinoin), and corticosteroid withdrawal.
- Sleep apnea: Associated with intermittent oxygen deprivation and altered intracranial pressure regulation.
- Other medical conditions: Chronic kidney disease, anemia, or thyroid imbalance may contribute in rare cases.
Symptoms of Idiopathic Intracranial Hypertension
IIH symptoms often mimic those of a space-occupying lesion in the brain. The intensity may fluctuate but typically includes:
Headache
The most common symptom—often severe, persistent, and worse upon waking or with eye movement. It may be accompanied by nausea or neck stiffness.
Visual Disturbances
- Transient visual obscurations: Brief episodes of blurred or lost vision, often lasting seconds.
- Double vision (diplopia): Usually due to sixth cranial nerve palsy.
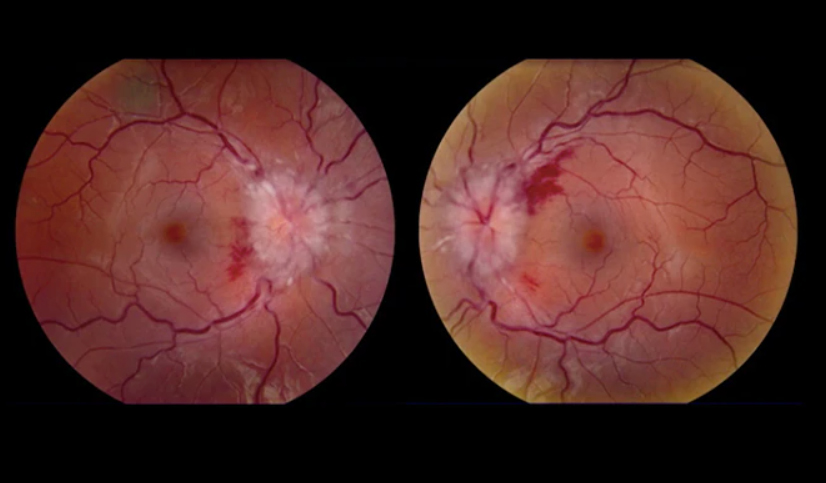
- Papilledema: Swelling of the optic nerve visible during eye examination.
- Progressive vision loss: Can occur in untreated or severe cases.
Pulsatile Tinnitus
A rhythmic “whooshing” sound in the ears synchronized with the heartbeat, caused by turbulent blood flow.
Other Symptoms
- Dizziness, light sensitivity, difficulty concentrating
- Shoulder or back pain in some patients
Diagnosis
Diagnosing IIH requires excluding other causes of raised intracranial pressure. Typical evaluation includes:
- Comprehensive history and exam: Assessment of symptoms, weight, medications, and comorbidities.
- Ophthalmologic evaluation: Eye exam for papilledema, visual field testing, and optical coherence tomography (OCT) to monitor nerve swelling.
- Neuroimaging: MRI of the brain with MR venography to rule out tumors, clots, or structural abnormalities; may show indirect signs such as posterior globe flattening or enlarged optic nerve sheath.
- Lumbar puncture (spinal tap): Confirms elevated CSF pressure (typically >25 cm H2O in adults) with normal fluid composition and can provide temporary symptom relief.
Treatment Options
The goals are to reduce intracranial pressure, preserve vision, and relieve symptoms. Management often combines lifestyle, medical, and surgical measures.
1. Lifestyle Modifications
- Weight reduction: Even modest loss (5–10%) can lower CSF pressure and improve symptoms.
- Diet and exercise: Low-sodium, balanced diet and supervised exercise to support weight loss.
2. Medical Management
- Carbonic anhydrase inhibitors (acetazolamide): First-line medication to decrease CSF production.
- Diuretics (e.g., furosemide): Sometimes used as adjunct therapy.
- Topiramate: May reduce CSF production and help with headaches and weight loss.
- Pain management: Analgesics for headache control, used cautiously to avoid medication-overuse headache.
3. Surgical Treatment
- Optic nerve sheath fenestration (ONSF): Relieves pressure on the optic nerve to protect vision.
- CSF shunting (LP or VP shunt): Diverts excess fluid to the abdomen when medical therapy fails.
- Venous sinus stenting: Considered when venous sinus narrowing contributes to elevated pressure.
Monitoring and Follow-Up
- Regular eye exams to monitor papilledema and visual fields.
- Periodic imaging or lumbar puncture as indicated.
- Prompt reassessment for any sudden visual changes.
Prognosis
With early diagnosis and appropriate management most people experience symptom relief and preserved vision. Delayed or inadequate treatment can lead to permanent optic nerve damage and chronic headaches. Weight management is the most effective long-term preventative measure.
Complications
- Permanent vision loss from prolonged optic nerve compression
- Chronic, debilitating headaches
- Shunt-related complications (infection, blockage, over-drainage)
- Medication side effects (fatigue, paresthesia, kidney stones)
Living with IIH
Successful management involves lifestyle changes, medication adherence, regular monitoring, and prompt reporting of visual changes. Patients should avoid excessive vitamin A, unnecessary steroids, and medications known to raise intracranial pressure. Emotional and psychological support can help cope with the chronic aspects of the condition.
