Ptosis surgery in Gurgaon
Drooping Eyelid
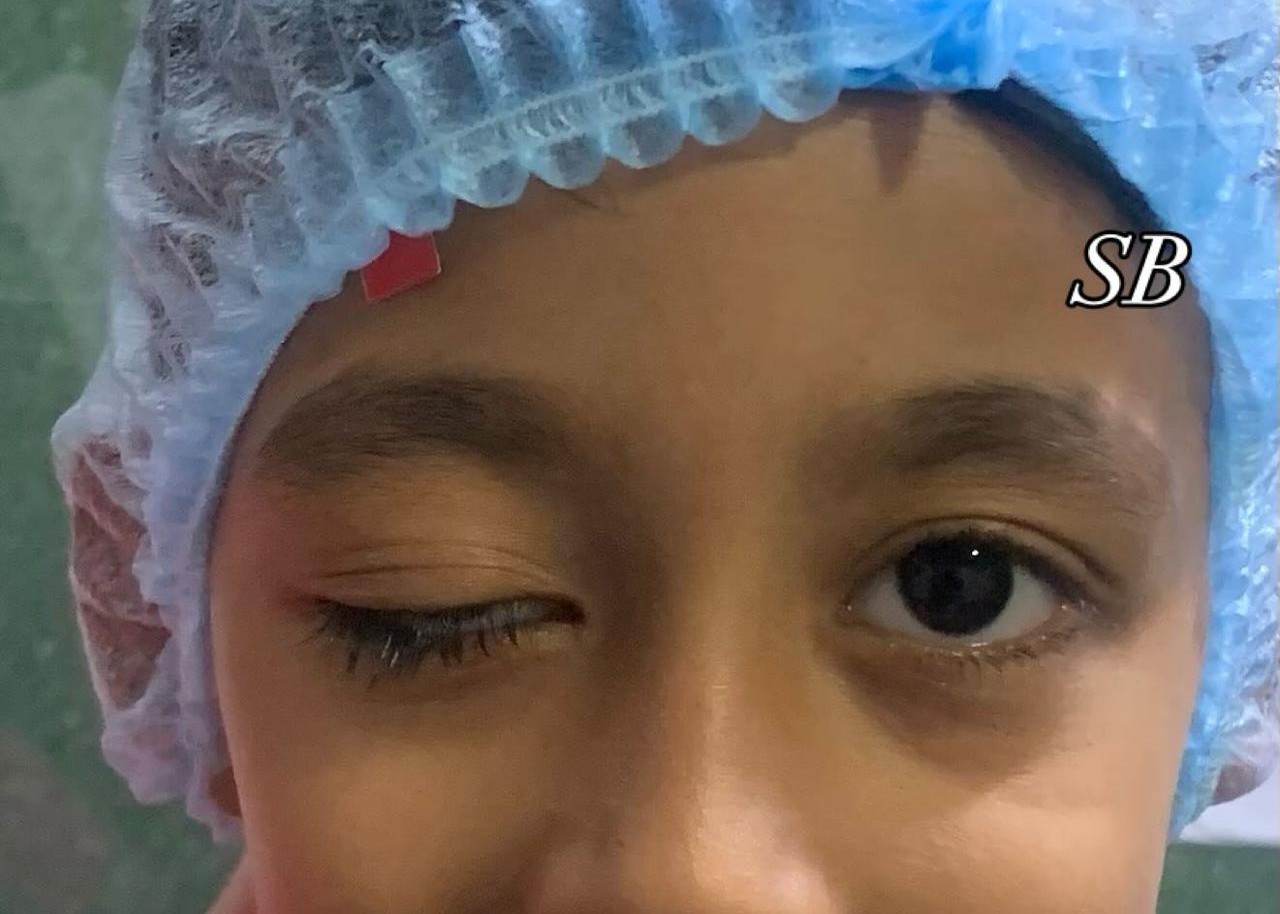
A drooping eyelid, medically known as ptosis, occurs when the upper eyelid falls lower than its normal position. This condition can affect one or both eyes and may range from mild to severe, sometimes covering the pupil and obstructing vision. Ptosis can appear at birth (congenital ptosis) or develop later in life (acquired ptosis).
While mild drooping is often harmless and mainly a cosmetic concern, significant or sudden drooping may signal an underlying medical problem that requires attention.
The eyelids are controlled by muscles—primarily the levator palpebrae superioris and Müller's muscle—which lift and maintain eyelid position. Any weakness, damage, or nerve dysfunction affecting these muscles can lead to drooping. Ptosis can occur gradually over time due to aging or appear suddenly as a result of trauma or neurological disorders.
Types of Drooping Eyelid
Congenital Ptosis
- Present at birth due to improper development of the levator muscle.
- Children with this condition may tilt their heads back or raise their eyebrows to see better.
- If severe, it can interfere with normal vision development and cause lazy eye (amblyopia).
Acquired Ptosis
Develops later in life and has several subtypes based on the cause:
- Aponeurotic Ptosis: The most common type in adults, caused by stretching or detachment of the levator tendon due to aging, eye rubbing, or long-term contact lens use.
- Neurogenic Ptosis: Caused by nerve problems that affect eyelid muscle control, such as Horner's syndrome, third nerve palsy, or myasthenia gravis.
- Myogenic Ptosis: Occurs when the eyelid muscles themselves are weak, as seen in muscular disorders like myotonic dystrophy.
- Mechanical Ptosis: Results from the eyelid being weighed down by excess skin, swelling, or a mass such as a cyst or tumor.
- Traumatic Ptosis: Develops after injury or surgery that damages the muscles or tendons lifting the eyelid.
Common Causes of Drooping Eyelids
- Aging (loss of muscle strength and elasticity)
- Congenital muscle abnormality
- Nerve damage (e.g., from stroke or diabetes)
- Eye surgery or trauma
- Neuromuscular disorders (e.g., myasthenia gravis)
- Tumors or swelling in the eyelid or orbit
- Chronic eye rubbing or long-term contact lens use
Symptoms of Ptosis
The primary sign of ptosis is a visibly drooping upper eyelid, but other symptoms can accompany it:
- Partial or complete covering of the pupil
- Difficulty keeping the eye open
- Eye fatigue or strain, especially when reading or watching TV
- Frequent raising of eyebrows to lift the eyelid
- Head tilting backward to improve vision
- Watery or dry eyes due to poor lid closure
- Uneven eyelid height (asymmetry between eyes)
In children, untreated ptosis can interfere with vision development, leading to lazy eye (amblyopia) or astigmatism.
Diagnosis
A complete eye examination by an ophthalmologist or oculoplastic surgeon is essential for accurate diagnosis. The evaluation typically includes:
- Visual Acuity Test: To check for any vision impairment.
- Eyelid Measurement: Assessing the height and strength of the levator muscle.
- Slit Lamp Examination: To evaluate the front structures of the eye.
- Neurological Assessment: If nerve-related causes are suspected.
- Tensilon Test (Edrophonium Test): Used when myasthenia gravis is suspected.
- Imaging Tests (CT or MRI): To rule out tumors or nerve compression if the cause is unclear.
Treatment Options for Drooping Eyelid
Treatment depends on the severity of the drooping and its underlying cause.
1. Observation
If the drooping is mild, doesn't affect vision, and is primarily cosmetic, regular monitoring may be sufficient. Children with mild congenital ptosis are also monitored to ensure vision develops normally.
2. Non-Surgical Treatments
- Prescription Eye Drops: Certain medications like oxymetazoline 0.1% (Upneeq) can temporarily lift the eyelid by stimulating MĂĽller's muscle.
- Treating the Underlying Cause: Managing conditions like myasthenia gravis or diabetes can help improve ptosis symptoms.
3. Surgical Treatments
When ptosis interferes with vision or causes significant asymmetry, surgery is usually recommended.
- Levator Resection (Levator Advancement): The surgeon shortens or reattaches the levator muscle to lift the eyelid to a normal position. Commonly used for mild to moderate cases.
- Frontalis Sling Surgery: For severe ptosis or poor levator function, a small sling (using silicone or other material) connects the eyelid to the forehead muscle, allowing the patient to raise the lid by moving their brow.
- MĂĽller's Muscle-Conjunctival Resection (MMCR): A minimally invasive procedure performed from the inside of the eyelid, suitable for mild ptosis with good muscle strength.
Recovery and Aftercare
After ptosis surgery, recovery is generally smooth with proper care:
- Mild swelling or bruising may last a few days.
- Use cold compresses to reduce swelling.
- Apply antibiotic ointment as prescribed.
- Avoid strenuous activities or rubbing the eyes for 1–2 weeks.
- Follow-up visits ensure proper eyelid height and symmetry.
Most patients experience immediate improvement in eyelid position and vision clarity after surgery.
Possible Complications
While ptosis treatment is generally safe, potential risks include:
- Over- or under-correction of eyelid height
- Asymmetry between the two eyelids
- Dry eyes due to incomplete eyelid closure
- Infection or temporary swelling
- Recurrence of drooping over time
These issues can often be corrected with minor adjustments or revision procedures.
Prevention and Early Detection
While not all cases can be prevented, you can reduce the risk or delay the onset by:
- Avoiding frequent eye rubbing
- Protecting eyes from injuries
- Managing chronic conditions like diabetes or neurological disorders
- Seeking early medical advice for sudden or progressive drooping
When to See a Doctor
You should consult an ophthalmologist if:
- The eyelid drooping occurs suddenly or worsens rapidly
- It blocks part of your vision
- It's accompanied by double vision, headaches, or facial weakness
- A child's eyelid covers the pupil or causes abnormal head posture
